
Sitagliptin Dose Adjuster
Dose Calculator
Sitagliptin phosphate is a prescription medication that belongs to the DPP-4 inhibitor class, used to improve blood‑sugar control in adults with type 2 diabetes. It works by blocking the enzyme dipeptidyl‑peptidase‑4, which in turn raises levels of incretin hormones that help the pancreas release insulin after meals. If you’re curious about Sitagliptin phosphate, here’s the lowdown.
Key Takeaways
- Sitagliptin phosphate boosts insulin release by inhibiting the DPP‑4 enzyme.
- It’s absorbed quickly, reaches peak blood levels in about 1‑4hours, and has a half‑life of roughly 12hours.
- The drug is eliminated primarily through the kidneys; dose adjustments are required for renal impairment.
- Common side effects include nasopharyngitis, headache, and mild gastrointestinal upset.
- Unlike some diabetes agents, sitagliptin carries a low risk of hypoglycemia when used alone.
How Sitagliptin Works - The Mechanism of Action
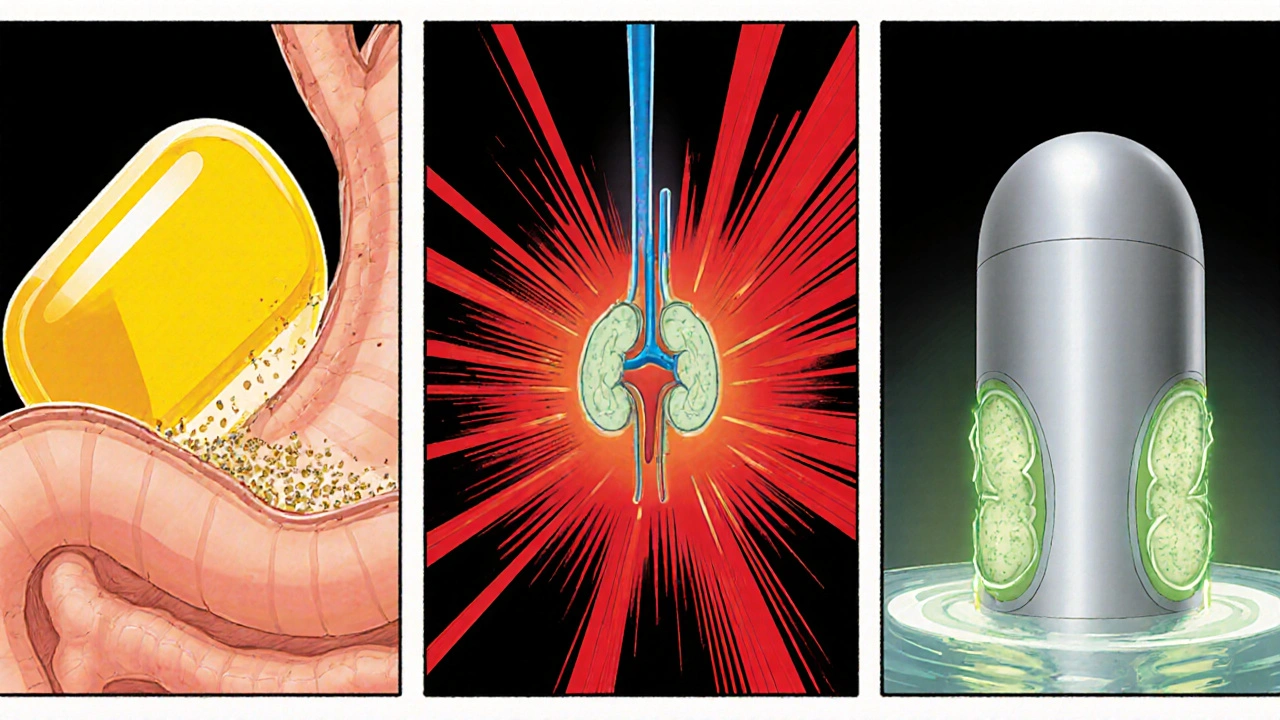
When you eat, your intestines release hormones called incretins, chiefly glucagon‑like peptide‑1 (GLP‑1) and glucose‑dependent insulinotropic polypeptide (GIP). These hormones tell the pancreas to secrete insulin and tell the liver to cut back on glucose output. A pesky enzyme-dipeptidyl‑peptidase‑4 (DPP‑4)-breaks down GLP‑1 and GIP within minutes.
Sitagliptin phosphate binds to the active site of DPP‑4, preventing it from degrading the incretins. The result? Higher circulating GLP‑1 and GIP levels, which enhance glucose‑dependent insulin release and suppress glucagon secretion. Because the effect is tied to meals, the drug works only when blood sugar starts to rise, which explains its low hypoglycemia risk.
Pharmacokinetics - What Happens After You Swallow a Tablet?
Absorption: Sitagliptin is taken orally, usually as a 100mg tablet. Bioavailability is about 87%, and food does not significantly affect uptake.
Distribution: The drug spreads throughout body fluids with a volume of distribution near 120L. Protein binding is minimal (<38%).
Metabolism: Unlike many oral agents, sitagliptin undergoes limited hepatic metabolism. Roughly 16% is metabolized via CYP3A4 and CYP2C8, forming inactive metabolites.
Excretion: About 79% of the dose is eliminated unchanged in the urine. The renal clearance mirrors the glomerular filtration rate, which is why practitioners adjust the dose for patients with reduced kidney function.
Half‑life: The elimination half‑life is approximately 12hours, supporting once‑daily dosing.
Clinical Use and Recommended Dosing
Guidelines in the United States, Europe, and Australasia recommend sitagliptin as monotherapy or as add‑on to metformin, sulfonylureas, or insulin. The typical adult dose is 100mg once daily with or without food.
Renal dose adjustments are essential:
- eGFR ≥50mL/min/1.73m²: 100mg daily
- eGFR 30-<50mL/min/1.73m²: 50mg daily
- eGFR 15-<30mL/min/1.73m²: 25mg daily
- eGFR <15mL/min/1.73m²: not recommended
In clinical trials, sitagliptin lowered HbA1c by an average of 0.7-0.9% when added to metformin, matching the efficacy of sulfonylureas but with a more favorable safety profile.
Safety Profile - What to Watch For
The most frequently reported adverse events (≥5% of users) include:
- Nasopharyngitis
- Headache
- Upper respiratory tract infection
- Gastro‑intestinal discomfort (nausea, diarrhea)
Serious but rare concerns involve pancreatitis, severe allergic reactions, and joint pain. Post‑marketing data have not confirmed a causal link to pancreatic cancer, but clinicians still monitor patients with a history of pancreatitis.
Because the drug does not directly stimulate insulin secretion, hypoglycemia is uncommon unless combined with insulin or a sulfonylurea.
Drug Interactions - Who Plays Well Together?
Sitagliptin’s limited metabolism means it has few interactions. However, be aware of these:
- Strong CYP3A4 or CYP2C8 inhibitors (e.g., ketoconazole, gemfibrozil) can raise sitagliptin plasma levels modestly.
- Diuretics may affect renal clearance; monitor renal function when combined with high‑dose thiazides.
- Insulin or sulfonylureas increase hypoglycemia risk-dose reduction may be needed.
Always review a patient’s full medication list, especially over‑the‑counter supplements that may impact kidney function.
How Sitagliptin Stacks Up Against Other DPP‑4 Inhibitors
| Drug | Typical Dose | Renal Adjustment | Metabolism Pathway | Notable Advantage |
|---|---|---|---|---|
| Sitagliptin | 100mg daily | Yes - see dosing table above | Minimal (CYP3A4/CYP2C8) | Well‑studied safety record |
| Linagliptin | 5mg daily | No adjustment needed | Primarily biliary excretion | Best for severe renal impairment |
| Saxagliptin | 5mg daily | Yes - reduce to 2.5mg if eGFR 30‑50 | CYP3A4 | Once‑daily with food |
| Alogliptin | 25mg daily | Yes - 12.5mg for eGFR 30‑50 | CYP2C8 | Low risk of drug‑drug interactions |
Practical Tips for Patients and Providers
- Check kidney function before starting therapy and at least annually thereafter.
- Encourage patients to take the tablet at the same time each day to maintain steady levels.
- Advise against abrupt discontinuation; taper only if serious adverse events arise.
- Combine with lifestyle measures-diet, exercise, weight management-for maximal HbA1c reduction.
- Document any signs of pancreatitis (persistent abdominal pain, nausea, vomiting) and stop the drug immediately if they appear.
Frequently Asked Questions
What makes sitagliptin different from metformin?
Metformin primarily reduces hepatic glucose production, while sitagliptin enhances insulin secretion after meals by protecting incretin hormones. They target different pathways, which is why they are often prescribed together.
Can I take sitagliptin if I’m pregnant?
Safety in pregnancy hasn’t been established. The FDA categorizes it as pregnancy‑category C, meaning risk cannot be ruled out. Discuss alternatives with your obstetrician.
How quickly does sitagliptin lower blood sugar?
Blood‑glucose reductions start within a week, with the full effect seen after 4‑6 weeks of steady dosing.
Is there a risk of weight gain?
Unlike insulin or sulfonylureas, sitagliptin is weight‑neutral for most patients. Small variations are usually due to diet or activity changes.
What should I do if I miss a dose?
Take the missed tablet as soon as you remember, unless it’s almost time for the next dose. In that case, skip the missed one-don’t double‑dose.





18 Comments
Raina Purnama
Oct 16 2025Thanks for the clear breakdown of sitagliptin’s mechanism. It’s helpful to see how DPP‑4 inhibition translates to better post‑meal glucose control. I’ll keep the renal dosing note in mind when reviewing patient charts.
April Yslava
Oct 18 2025Honestly, the pharma giants don’t want you to know that sitagliptin is just a cash cow for the big labs. They hide the fact that it manipulates your gut hormones to keep you hooked on their pills. Wake up, folks! The side‑effects list is a cover‑up, and the “low hypoglycemia risk” is just marketing hype. Keep your eyes open.
Rebecca Bissett
Oct 21 2025Wow!!! This article actually does a great job!! The way DPP‑4 is explained is sooo clear!!! I feel like I finally understand why my doctor chose sitagliptin!!
josh Furley
Oct 23 2025Interesting take, but let’s think about the bigger picture 🤔. Inhibiting an enzyme sounds simple, yet the downstream effects are a bit of a philosophical puzzle, don’t you think? The body’s feedback loops are like a maze.
😊Carissa Engle
Oct 25 2025Sitagliptin’s pharmacokinetics deserve a deeper look. First, the drug is absorbed almost completely, which means you get a predictable exposure each time you swallow a tablet. Second, the peak plasma concentration occurs within one to four hours, aligning nicely with post‑prandial glucose spikes. Third, the half‑life of roughly twelve hours allows for once‑daily dosing, simplifying patient adherence. Fourth, the minimal protein binding indicates that drug interactions through displacement are unlikely, but renal clearance dominates elimination. Fifth, because it is excreted unchanged in the urine, dose adjustments are mandatory for patients with impaired renal function, otherwise accumulation can happen. Sixth, the low affinity for cytochrome P450 enzymes reduces the risk of metabolic drug‑drug interactions, a point often overlooked. Seventh, the safety profile shows common adverse events such as nasopharyngitis, headache, and mild gastrointestinal upset, which are generally tolerable. Eighth, the risk of severe hypoglycemia is low when sitagliptin is used as monotherapy, but it can increase when combined with sulfonylureas or insulin, so clinicians must monitor glucose closely. Ninth, the drug does not significantly affect body weight, which is a benefit compared to some older antidiabetic agents. Tenth, the chemical stability of the tablet allows for flexible storage conditions, a practical consideration in many regions. Eleventh, patients should be counseled to take the medication with or without food, as food has negligible impact on bioavailability. Twelfth, real‑world data suggest that adherence improves when patients understand the mechanism, reinforcing the need for patient education. Thirteenth, clinicians should be aware of rare but serious adverse events such as pancreatitis, although the causal relationship remains uncertain. Fourteenth, the cost of sitagliptin can be a barrier for some, prompting the need for insurance navigation. Fifteenth, generic versions are now available, which may alleviate the financial burden. Sixteenth, overall, sitagliptin provides a valuable option in the therapeutic armamentarium for type 2 diabetes, especially for patients who cannot tolerate metformin or need an add‑on therapy with a low hypoglycemia risk.
Dervla Rooney
Oct 28 2025Good overview.
Johnny Ha
Oct 30 2025Yo, they’re hiding the truth about how these “miracle” pills keep the pharma oligarchy in power. If you’re not watching the fine print, you’re just another pawn.
Mary Cautionary
Nov 1 2025While the enthusiasm is noted, it is paramount to acknowledge that the clinical efficacy of sitagliptin, albeit modest, is supported by robust randomized controlled trials. The nuanced balance between glycemic benefit and safety profile warrants a discerning appraisal.
Crystal Newgen
Nov 4 2025I appreciate the neutral tone of this post; it’s useful for newcomers trying to understand diabetes meds without the hype.
Hannah Dawson
Nov 6 2025Neutral is fine, but the piece glosses over rare but serious adverse events like pancreatitis. Ignoring those risks can mislead patients who think it’s completely safe.
Victoria Unikel
Nov 8 2025i read this and it kinda helps me get why my doc gave me sitagliptin. seems easy to take and not many side effects.
Rama Hoetzlein
Nov 10 2025Simple explanations are fine, but the truth is deeper-these DPP‑4 inhibitors are part of a larger pharmaco‑economic agenda to keep us dependent on daily pills. The hormone modulation they cause is nothing but a calculated way to keep blood sugar just high enough to need more drugs. 🤔
Annie Tian
Nov 13 2025Great summary! This will definitely help patients feel more confident about their treatment options.
April Knof
Nov 15 2025Indeed, clarity is vital for patient empowerment. Knowing how sitagliptin works can improve adherence and outcomes.
Ellie Hartman
Nov 17 2025For anyone starting on sitagliptin, remember to check your kidney function before dosing. It’s a small step that makes a big difference in safety.
Jason Divinity
Nov 20 2025While the advice is sound, let’s not forget that renal dosing is just one facet of individualized therapy. A comprehensive review of comorbidities, concomitant medications, and patient preferences should guide the final decision.
andrew parsons
Nov 22 2025It is essential to underscore that, despite its favorable profile, sitagliptin must be prescribed judiciously. The clinician should evaluate the totality of evidence, including cardiovascular outcomes, before integrating it into a therapeutic regimen. Moreover, patient education regarding potential adverse effects, albeit infrequent, remains a cornerstone of responsible prescribing.
Sarah Arnold
Nov 24 2025Absolutely, proper prescribing and patient counseling are key. If you have any questions about dosing or monitoring, feel free to ask – happy to help! 😊